Evidence-informed Home Health Management of Total Hip Arthroplasty
By: By Babatope Olusina, PT, DPT and Olaide Oluwole-Sangoseni, PhD, DPT, MSc.
Osteoarthritis is a degenerative joint disorder that affects the articular cartilage, underlying bone, and surrounding soft tissues. It is the most common form of joint disease in the United States (US), with an estimated prevalence of 27 million people,1 with an occurrence of about 10% in men and 13% in women, over the age of 60 years. 2 Hip osteoarthritis accounts for about 70% of total hip arthroplasties (THA) that are performed in the US due to severe pain, which limits the individual’s functional mobility and negatively affects his/her activities of daily living (ADLs), eventually limiting his/her participation in work and leisure activities. 3 Other indications for THA include but are not limited to trauma and osteonecrosis of the femoral head.4
THA is the surgical replacement of the natural hip joint with a prosthesis. 3 The first THA procedure was completed in the US in 1969 and as the procedure has grown in incidence, the technique has evolved and its efficacy has improved. 2,4 A 2010 prevalence study estimated 2.34% of individuals over the age of SO years in the United States have had THA, corresponding to 2.5 million people (1.4 million women). 4 A detailed breakdown of their study revealed a prevalence of 0.58% at age SO years, increasing to 1.49% at sixty years, 3.25% at seventy years, 5.26% at eighty years, and 5.87% at ninety years of age.4 The original or more popular technique is the posterior or posterolateral approach, with its associated precautions (no hip flexion above 90 degrees, no adduction beyond the midline, and no internal rotation of the surgical hip joint).
In the 1980s, an anterior approach was developed and gained popularity because of improved early outcomes in terms of pain and early functional recovery. 5 Hip hemiarthroplasty is the surgical removal of one of the components of the hip joint, most often the femoral head. Although it is less invasive, the Physical Therapy assessment and management will follow a similar path as for a THA.
Home health physical therapists (HHPT) are part of the multidisciplinary team-approach called upon to manage these patients upon their return home. Orthopedic surgeons seek the involvement of physical therapists (PT), as movement specialists, to facilitate the recovery and rehabilitation of THA patients to maximize their return to full function and participation in the activity. In consultation with the orthopedic surgeons, our home health agency established protocols that can be customized to fit the individual patient’s desired outcomes and surgeon’s preferences. These protocols guide the first few weeks of in-home rehabilitation before the transition to outpatient physical therapy. As a HHPT with a weekly caseload of about 50 percent of total hip and total knee arthroplasty patients, I recognize that no two patients’ status post-THA is the same.
The Medicare home health Conditions of Participation (CoP) require that a comprehensive assessment of each patient be performed by the admitting clinician to start the episode of care. This assessment includes the patient’s past medical history (PMH); a complete review of the patient’s medications, including any changes in dosage and patient’s response; and the integumentary assessment, all of which go into the process of formulating the patient’s plan of care.
Because most home health patients have multiple diagnoses, the evaluating PT incorporates the patient’s past medical/surgical history and the patient’s prior level of function into his/her physical therapy plan of interventions. A detailed assessment of the patient’s home is an essential aspect of the initial visit, as safety hazard/fall risks can be identified, and safety education and recommendations can be immediately communicated to the patient and their caregivers. The purpose of this case report is to highlight the physical therapy management of a THA in the home health setting with a focus on adapting exercise program based on pain and muscle fitness indices.
Case Presentation:
The patient is an 81-year-old female, retired nurse admitted to HHPT following right THA revision with weight-bearing as tolerated precautions. She resides alone in a single level house in a 55+ Age-in-Place community. Before this surgery, she was fully independent with all of her functional mobility, occasionally using a standard straight cane for ambulation. She was independent with all activities of daily living (ADL)s and was active in her community, participating in group exercise sessions every week.
Past Medical History:
Her PMH was significant for multiple comorbidities: hypertension, atrial fibrillation, type 2 diabetes mellitus, anxiety, neuropathy, general osteoarthritis, vertigo, history of lumbar laminectomy and fusion in 2017, reflux disorder, cystocele with prolapse, and recent urinary tract infection. Initial THA was performed in 2002; she had a dislocation in 2017, which resulted in persistent hip joint pain afterward.
The patient stated her goal is to return to walking independently without the walker.
Objective Examination and Assessment
Physical Status:
On examination, “Nanette”(a pseudonym) was alert and oriented to person, place, and time, and able to follow a multi-level command. She presented with hypomobility of the hip joint and weakness of the proximal muscles of the surgical lower extremity. She required contact guard/minimal assistance to assist her right lower extremity into the bed during bed mobility assessment. She required close stand-by-assistance of the therapist for sit to/from stand and bed to/from chair transfers due to She was dependent on a rolling walker for ambulation, with forward-flexed trunk posture over the device, using a 2-point antalgic gait pattern. The Timed Up and Go test (TUG) was performed, with the “Nanette” requiring 36 seconds to complete. 6 A time greater than 20 seconds is indicative that the patient is dependent on transfers and confirms homebound status. 6 The family had hired a private duty company to provide personal care assistance for several hours during the day to assist her in the first 3 weeks.
Integumentary:
Because the initial home PT evaluation was on the same day as the nursing start of care (SOC) visit, PT evaluation referred to the nursing integumentary assessment. However, the physical therapist assessed the surgical incision on each subsequent visit, per our agency protocol, performing dressing changes when needed. The status of the wound was documented and presented at the interdisciplinary case conference with the registered nurse as required.
Pain:
Per Medicare CoP, Nanette’s pain was evaluated on the initial examination and all subsequent visits, using a numeric pain rating scale (0-10) and verbal description. She rated her pain at level 5/10; her goal was to be pain-free by discharge. The expectation was a gradual decrease in the pain level, and any movement in the other direction and/or a new type of pain warrants additional evaluation.
Clinical Impression:
Based on the hypomobility of the hip joint and weakness of the proximal muscles of the hip and pelvis, the International Classification of Functioning, Disability and Health (ICF) model diagnosis of M25.651 or 652 (stiffness of hip joint, not elsewhere classified) was made.
Plan of Care
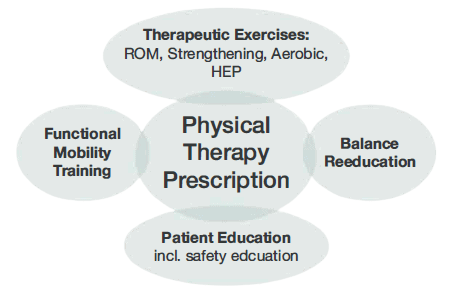
It was determined that Nanette would benefit from a skilled PT intervention frequency of 2 times per week for 4 weeks. Her exercise prescription consisted of joint mobilization, ROM and strengthening exercises, instruction in a home exercise program (HEP), functional mobility training (including bed mobility, transfer, and gait training), balance reeducation, equipment training, safety education, to progress to independence in all areas (Figure 1).
Figure 1: Physical Therapy Plan of Care
Since the pain was the chief complaint, it was used as one of the outcome measures. Pain medication was to be taken an hour before the PT session. The patient’s pain level was expected to decrease to level 1/10 at discharge.
Therapeutic exercises on the day of the examination consisted of:
Isometric contraction of the quadriceps and bilateral gluteal muscles sustained for 5 seconds or until fatigue.
Isotonic exercises, including hip abduction (in standing), hip/knee flexion (in supine via heel slide) and knee extension (in sitting), ankle dorsiflexion and plantarflexion (in supine), up to 15 repetitions or until fatigue, using BORG rate of perceived exertion (RPE) score with a target score of 14 on the 6-208 scale.8 The PT’s focus was on increasing muscle endurance using a high repetition approach. The patient’s positioning during exercise was modified in sitting and standing due to a history of chronic acid reflux; she was unable to tolerate supine lying.
Exercise progression/upgrade included gradual addition of hip flexion, abduction, and extension in standing for muscle strengthening-an upgrade of knee flexion, ankle dorsiflexion, and plantarflexion in standing using gravity and bodyweight resistance. Exercise intensity was based on RPE, and the type of exercise was the final two weeks to include external hip rotation in the supine position.
Home Exercise Program (HEP): The patient was instructed to perform the aforementioned exercises as her HEP 2-3 times daily on the days that the PT is not scheduled, to maximize her progress and to progress her towards her stated goal. Nanette’s adherence was crucial to her overall recovery, stated personal goal, and physical therapy outcome. HEP adherence was monitored through direct open-ended questions and requested demonstrations during subsequent visits. Nanette was provided education to encourage cooperation with the overall plan of care.
Functional mobility training included bed mobility training with safety instructions given to ensure the patient adhered to the THR precaution during supine to sit and sit to supine mobility. Transfer training included regular sit to/from stand, toilet transfers, shower and tub transfer training, and, later, car transfer training in preparation for discharge. The patient received gait training with the rolling walker, with verbal and visual instructions provided to address the deficits and impairments noticed during her initial examination. This patient received instructions for postural reeducation, and to increase stance time and the amount of weight-bearing in her right LE. As her pain subsided 2-3 points, and her right LE muscle strength improved, she was progressed to the use of a standard cane first on level surface, and later on uneven surfaces. Just before discharge, the patient was progressed to gait training without an assistive device.
Balance reeducation in standing started with transitional weight-shifting patterns in the sagittal and coronal planes. The verbal emphasis was on maintaining upright trunk posture, increasing stance time on the surgical leg, and improving the amount of weight-bearing. The first progression of this was to perform the same activities without upper extremity support. The next progression was the use of transitional stepping patterns in the sagittal and coronal planes. These activities were performed to improve the muscle stabilization action around the replaced hip joint, as well as improve the patient’s confidence in the ability of the surgical hip to sustain her weight. This is essential in the progression of gait training from a walker to a cane, and eventually to ambulating without a device.
Patient Education Patient education was a multi-pronged approach. The patient demonstrated a high level of health literacy; therefore, patient education was a multi-pronged approach. The PT provided education about Nanette’s THA precautions, with emphasis on observing these precautions as she goes through her day-to-day activities. Nanette’s precautions included avoiding turning towards the affected side, sitting in a low chair, and during supine to/from sitting, as these are some of the times when a patient is most likely to break the precautions. Safety education was provided in direct correlation to the safety hazards identified during the initial examination visit and other sessions. Nanette had area rugs in her walking path and a narrow path to her side of the bed. The PT provided suggestions and education regarding fall risks and prevention. Her bed was rearranged to allow a wider path to fit the walker. Area rugs were removed throughout the home. Also, caregivers (daughter and paid caregiver) were provided with education on a variety of topics, including Nanette’s home exercise program, signs, and symptoms of a deep venous thrombosis (DVT), pain medication management, the application of cold modalities for pain management, and if and when to seek medical attention. Researchers have suggested that there is an emergency room visit rate of about 13.4% in the first 90 days following THA, and the most frequent reasons are swelling (15.6%) and uncontrolled pain (12.8%).7 A study by Saleh et al documented these same common surgery-related reasons accounted for emergency room (ER) visits in about 35% of patients.9 These studies underscore the role of home health professionals in patient education regarding the careful assessment and management of swelling and pain in this population, as well as identifying patients that need to be referred to the ER for further evaluation immediately. This PT utilizes Wells’ Criteria for DVT10 as a clinical tool whenever there is concern about a possible DVT.
Outcomes
The patient achieved independence with her bed mobility by the first session of week 2 (3rd visit), and independence with her sit to/from stand and chair to/from bed transfers by the end of the second week (4th visit). She demonstrated independence with her shower stall and tub transfers by the third week (6th visit) and independence with car transfer in the 4th week. The patient progressed to gait training with a standard cane by the 3rd week. She had progressed to independence with gait training on level and uneven surfaces, including on her inclined driveway and to her community mailbox, which is about 450 feet away from her front door, with a numeric pain score of 0/10. Her functional score improved from 36 seconds at initial evaluation to 12 seconds using the TUG test. This score correlates with independence in all transfers and activities of daily living. Her right hip muscle strength had improved to 3+/5, and the patient demonstrated independence with her HEP. Nanette had achieved pain-free status by the final visit.
Discussion
This patient presented with several impairments that created limitations at the body function level as well as at the activity and participation level, 11,12 as laid out above with the ICF model.
The HHPT used his/her expertise to provide an individualized, person-centered, evidence-informed treatment in the management of this patient. The plan of care was based on the interdisciplinary protocol developed by the surgeon and the home health agency, to help achieve the goals she stated as important to her. Nanette was motivated to return to driving and get back to her normal social life with her friends in the 55+ Age-in-Place community where she resides. The patient had multiple episodes of elevated blood pressure that warranted the notification of her primary care physician (PCP). To err on the side of caution, our home health agency policy requires physician notification for any systolic above 150 and diastolic above 90mmHg. Although her PCP decided not to take any immediate action, her blood pressure was carefully assessed at the start of each visit and response monitored throughout the interaction. The patient had a medical history of anxiety, which sometimes played a role in her exercise response and feedback to the therapist, especially related to her RPE rating and response. She required frequent reassurance, and it was well managed afterward.
Further, consistent with her medical history, constant adjustments had to be made based on observations and findings at the beginning of each visit. Some of her exercises were modified, considering her history of back pain and surgery to avoid aggravating old symptoms. She received a reiteration of education regarding home safety and community re-entry in the last week of the HHPT visit.
Nanette was discharged from home health nursing services in her second week and was discharged to outpatient therapy upon completion of her 8th and final visit. She planned to start driving, first inside her community, once she was released from home health services. An anonymous satisfaction survey was mailed to her by the agency after discharge, and she expressed her satisfaction to the therapist on her last visit, showing how quickly she was progressed to independence with physical therapy. This case report demonstrates a successful progression of an individual with a posterior approach THA from acute care to return to community living through a three-week course of HH services.
About the Authors
Babatope Olusina, PT, DPT, Certificate of Advanced Competency in Home Health (APTA Home Health Section). He is a member of the APTA and Home Health section. Dr. Olusina now works for a home health agency in Richmond, VA, but previously owned and ran a Contract Therapy Staffing Company.
Dr. Olaide Oluwole-Sangoseni, PhD, DPT, MSc, GCS, is an associate professor of physical at Maryville University of St. Louis. She is a Board Certified Geriatric Specialist and a home health PT. Dr. Sangoseni is an advanced physical therapy clinical specialist degree in neuro-orthopedics from the University College London, England. She is an APTA credentialed clinical instructor. She can be reached at [email protected].
References
Lespasio MJ, Sultan AA, Piuzzi NS, et al. Hip osteoarthritis: a primer. Perm J. 2018;22:17-084. DOI: https://doi.org/10.7812/TPP/17-084
United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Fourth Edition, 2020. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed on June 15, 2020
Siopack JS, Jergesen HE. Total hip arthroplasty. West J Med. 1995;162:243-249, 1995
Kremers HM, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacements in the United States. J Bone and Joint Surgery. 2015: 97(17): 1386-1397
Wang Z, Hou JZ, Wu CH, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res. 2018;13(1):229. Published 2018 Sep 6. doi:10.1186/s13018- 018- 0929
Centers for Disease Control and Prevention: National Center for Injury Prevention and Control. STEADI Tools. https://www.cdc.gov/steadi/pdf/ TUG_Test-print.pdf. Published 2017. Accessed on June 20, 2020
Kelly MP, Prentice HA, Wang W, Fasig BH, Sheth DS, Paxton EW. Reasons for ninety-day emergency visits and readmissions after elective total joint arthroplasty: results from a US integrated healthcare system. J Arthroplasty. 2018;33(7):2075-2081. doi:10.1016/j.arth.2018.02.01 O
Williams N. The Borg Rating of Perceived Exertion (RPE) scale. Occupational Mede.2017; 67(5):404-405, https://doi.org/10.1093/occmed/kqx063
Saleh A, Faour M, Sultan AA, Brigati DP, Molloy RM, Mont MA. Emergency department visits within thirty days of discharge after primary total hip arthroplasty: a hidden quality measure. J Arthroplasty. 2019;34(1):20-26. doi: 10.1016/j.arth.2018.08.032
Wells PS, Anderson DR, Rodger M, et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003 Sep 25;349(13):1227-35.
Klapwijk LC, Mathijssen NM, Van Egmond JC, Verbeek BM, Vehmeijer SB. The first 6 weeks of recovery after primary total hip arthroplasty with fast track [published correction appears in Acta Orthop. 2018 Feb;89(1):140]. Acta Orthop. 2017;88(2):140-144. doi:10.1080/17453674.2016.1274865
Bahardoust M, Hajializade M, Amiri R, Mousazadeh F, Pisoudeh K. Evaluation of health-related quality of life after total hip arthroplasty: a case-control study in the Iranian population. BMC Musculoskelet Disord. 2019;20<1>:46. Published 2019 Jan 31. doi:10.1186/s12891-019-2428-0
Evidence-informed Home Health Management of Total Knee Arthroplasty
By: By Babatope Olusina, PT, DPT and Olaide Oluwole-Sangoseni, PhD, DPT, MSc.
Osteoarthritis (OA) is a degenerative joint disorder that affects the articulating bones, the articular cartilage, and surrounding soft tissues. Other causes of joint pain and degeneration include rheumatoid arthritis (RA), osteonecrosis, post-traumatic degenerative joint disease, and other pathologic conditions. While joint pain is usually the first sign that prompts the decision to seek medical attention1, other symptoms soon develop, including but not limited to joint hypomobility and muscle weakness. The progression of the disease results in the development of functional limitations such as difficulties with transfers, gait abnormality, stair management, and completing activities of daily living (ADLs), eventually having negative impacts on work, pleasure, and quality of life.
The knee joint is the largest weight-bearing joint in the body, and chronic knee pain has been listed as a “leading cause of musculoskeletal disability in the United States (US)”. 2 Total knee arthroplasty (TKA) is the surgical replacement of the natural knee joint with a prosthesis. It was the first performed in the US in 1968, and with ongoing advances in the technique and materials used, significant progress has been made in its effectiveness and success rate. A 2010 prevalence study of TKA by Kremers el al3 estimated 1.52% in the entire US population, and 4.55% in those over the age of 50 years, have had TKA. Prevalence is higher in women as compared with men, and it increases with age. Inacio et al4 projects that the number of TKAs performed in the US will increase by the year 2050 to a prevalence of 2.58%, amounting to 2,854 procedures per 100,000 US citizens. Partial knee replacement is often performed when the degenerative changes are confined to a particular compartment of the knee and mostly in the younger patient. The PT management is similar to that of a TKA, as described later in this study.
Physical therapy (PT) plays a major role in the initial conservative management of the knee pain before TKA, not only for pain management but also to improve function and decrease the limitations afflicted by the condition. Following a TKA, the home health physical therapist is part of the multidisciplinary team approach that manages the patient upon discharge home. Our Home Health Agency (HHA) has developed protocols to manage these patient populations effectively. Based on previously established protocol with the referring Orthopedic Surgeon, a registered nurse (RN) completed the initial visit, performing a comprehensive assessment of the patient, including the past medical history (PMH), assessment and care of the surgical incision, medication review/training, and the OASIS elements. This HHA also has established protocol with other Orthopedic Surgeons where the PT is the admitting clinician. The initial PT evaluation consists of a detailed musculoskeletal assessment of the patient, a review of the patient’s PMH, gait and balance evaluation, and a home safety evaluation. A PT plan of intervention is formulated to address noted impairments and functional limitations, with the patient’s self-stated goal as the endpoint.
The purpose of this case report is to highlight the physical therapy management of TKA in the home health setting.
Case Presentation:
The patient is a 50-year-old female office worker referred to home PT and Nursing following a right TKA revision due to instability and eventual failure of hardware. She resides with her husband in a single-level house, with 8 entrance steps, and she was fully independent with all of her functional mobility, including ambulating without an assistive device, but she was limited by right knee pain and the knee “locking up”.
Past Medical History:
Her PMH was significant for multiple comorbidities: Significant for Hypertension, Diabetes Mellitus, Hyperlipidemia, Asthma, Anemia, Cervical spine stenosis, Elevated Hemoglobin, Ehlers-Danlos syndrome, Depression, Metabolic syndrome, and Premature Ventricular Contraction (PVC). Her past surgical history is significant for Bilateral TKA, Anterior cervical discectomy with fusion, and Caesarean Section.
Medications:
Acetaminophen, 500mg, 1 tab Q 4 hours as needed.
Apixaban, PO, 2.5mg, 1 tab, twice daily
Benadryl, 25mg, 1 cap daily
Celebrex, 100mg, 1 cap twice daily
Vitamin D3, 125mcg, 1 tab daily
Crestor, 5mg, 1 tab daily
Doxycycline Monohydrate, 40mg, 1 cap daily
Ferrous Sulfate, 325mg, 1 tab twice daily
Lisinopril-HCTZ, 20-12.5mg, 1 tab daily
Metformin, 500mg, 1 tab twice daily
Oxycodone, 5mg, 1 tab Q 4 hours, as needed
Senna with Docusate Sodium, 8.6mg-50mg, 1 tab daily
Singulair, 10mg, 1 cap twice daily
Vitamin B12, 1,000mcg, 1 tab daily
Cephalexin, 500mg, 1 tab 3x daily (started on 12/27/20)
Objective Examination and Assessment
Physical Status:
During her initial evaluation completed on 12/26/20, Valerie presented an alert and oriented to person, time, and place, and able to follow multi-level commands. She presented with hypomobility of her right knee (flexion ROM of 81 degrees and extension at negative 6 degrees) and weakness in her right quadriceps and hamstring muscle strength (2+/5 on the Manual Muscle Testing grade). She had difficulty with her bed mobility requiring close stand-by assistance, and she required supervision for her transfers. She was dependent on a pair of axillary crutches for ambulation using a 2-point gait pattern. She also used an antalgic gait pattern and exhibited poor arthrokinematics in the right knee. Her balance was assessed with the Timed Up and Go test (TUGT)5, with a score of 17 seconds; this identified her as having a high risk of falls.
Integumentary:
The patient’s right knee surgical incision was covered with “Aquacell”, a non-removable dressing on the day of PT evaluation. It was removed by skilled nursing during the subsequent visit on 12/29/20. PT assessed the patient’s surgical incision during all follow-up visits, for signs and symptoms of infection. This is part of agency protocol that all clinicians will assess surgical incision and document appropriately; coordination of care is performed weekly with the RN case manager.
Pain:
The patient’s pain level and description were assessed and documented during the initial PT evaluation and subsequent visits. The PT provided education to the patient and her husband regarding pain management strategies with her prescription analgesics, cryotherapy, and movement.
Clinical Impression:
Based on the hypomobility of her Right knee joint and the weakness of her right hamstring and quadriceps muscles, the International Classification for Functioning, Disability and Health (ICF) model ICD diagnosis of M25.661 (stiffness of right knee, not elsewhere classified), was made.
Plan of Care
PT determined that patient will benefit from skilled intervention with a frequency of 3 times per week for 3 weeks, per previously established protocol with referring surgeon. The intervention included therapeutic exercises (including a range of motion [ROM], strengthening exercises, and joint mobilization), functional mobility training (including bed mobility, transfer, gait, and stair training), instruction in-home exercise program, balance reeducation, safety education, equipment training, patient and caregiver education, and training, to progress her to independence in all areas.
Patient has a diagnosis of Ehlers-Danlos Syndromes (EDS)6, a connective tissue disorder with joint hypermobility as one of its primary symptoms. Her therapeutic exercises, especially her ROM, were modified acccording to her symptoms and feedback. Therapeutic exercises prescription and progression was developed based on the phase of her rehabilitation, described as follows:
Days 1-10 acute phase (with emphasis on ROM, isometric and isotonic exercises)
Right quadriceps isometric contraction in a supine positon, sustained for 5 seconds, 10 repetitions;
Isometric exercises in supine and sitting position including hip flexion, knee flexion and extension (short and long arc quads), ankle doriflexion, and plantarflexion, 10 repetitions;
Right knee flexion and extension active range of motion (AROM) and active-assisted range of motion (AAROM) in supine and sitting positions, 5 repetitions of in each direction, or fewer based on patient’s pain or feedback.
Progression to the next phase (sub-acute) was based on decreased in overall pain and joint effusion and improvement in Right LE muscle strength.
Days 11-21 the sub-acute phase (with progression to advancing ROM, strengthening exercises, and joint mobilization)
Right knee AROM/AAROM/passive range of motion (PROM) to facilitate full extension ROM and maximum flexion ROM, 5 repetitions in each direction.
Grade I knee joint mobilization in sitting and supine positons, to improve flexion and extension ROM, with close monitoring of her pain and to prevent hypermobility in either direction, 1-2 repetitions.
Strengthening exercises using gravity and body weight for resistence, including hip flexion, extension, and abduction; knee flexion and extension (shot and long term arc quads); standing ankle dorsiflexion and plantarflexion, 2 x 10 repetitions.
Use of eccentric muscle action to facilitate improvement of VMO strength, due to patient’s mild extension lag during SAQ and LAQ, 10 repetitions.
Home exercise program (HEP) – the patient was instructed to perform her HEP 2-3 times daily. HEP was upgraded from Phase 1 to Phase 2 as the joint effusion and pain decreased, the right LE muscle strength and coordination improved.
Functional mobility training – The therapist provided verbal and visual instructions to the patient to quickly teach bed mobility and transfer techniques to progress her independence in both areas. Gait training with a pair of axillary crutches, emphasizing the proper use of the 2-point gait pattern and ensuring the crutches support the right LE, was performed. PT emphasized the need to increase right knee flexion ROM during the non-weight bearing phase of gait and facilitate full knee extension at heel strike. She was started on gait training with a one-handed device by the end of the second full week and progressed to independence by the end of her 3 weeks of home PT.
Balance reeducation – transitional weight-shifting patterns in the anteroposterior and lateral directions in standing, facilitating increased weight bearing on the surgical leg. Later progressed to using a narrow base of support (BOS) in a modified tandem position, where she initially required contact guard assistance and later progressed to supervision level.
Patient education: PT provided detailed instruction to the patient and her husband regarding pain and joint effusion management, signs and symptoms of DVT and infection at the wound site, and edema management. Patient education was specific to the home exercise program. Several studies have identified pain, fear of DVT, and edema as the most common reasons patients visit to the emergency room. (5-7) Therefore, our agency emphasizes patient education regarding symptoms management and patients’ expectations of their recovery roadmap. Safety education was provided, emphasizing the patient safely navigating her house with 2 cats and 2 small dogs underfoot. Her husband was instructed to, and he ensured a clear path to the bathroom from her bed, and he provided assistance that patient required for her first few shower transfers. During her fourth HHPT visit on 1/4/21, the patient reported feeling sick, dizzy, and nauseous after completing her supine and sitting exercises. Her vital signs were initially checked at the time of the therapist’s arrival, and they were within normal for the patient. She was assisted back to the couch, and her vital signs were re-checked; her blood pressure was now 91/53 mmHg, pulse was 94 beats per minute, and respiratory rate was 20 per minute, and her oxygen saturation was 98%. Further, the patient was diaphoretic and quite anxious. The PT re-assured the patient and provided moving air to cool her down. After about 5 minutes in a supine position with her lower extremities elevated, she reported feeling “somewhat better”. Her vital signs were re-checked – BP was 91/59 mmHg; pulse at 93 beats per minute; respiration at 16 per minute, and oxygen saturation at 98%. The patient’s surgeon’s office was contacted and informed about the incident. Her primary care physician (PCP) was also informed per the patient’s request. Both physicians agreed with the therapist that the patient did not require emergency care because her oxygen saturation remained within normal range, and she recovered in terms of her subjective feeling. PT ruled out possible Pulmonary Embolism (PE) using Well’s Criteria and ruled out possible DVT. She subsequently missed the next scheduled session on 1/6/21; even though she reports feeling better, she asked for another day to rest before resuming PT. She had a follow-up appointment with her primary care physician on 1/11/21 and was started on an iron supplement for postoperative anemia.
Outcomes
The patient completed 8 of 9 planned HHPT visits, and she had progressed to independent bed mobility and transfers by her third visit on 12/30/21. By the end of the 3rd week her progress was as follows:
ambulating independently without an assistance device for 180 feet inside her house and with one crutch on uneven surfaces
modified independent level managing her 8 entrance steps
right knee AROM at 0-122 degrees.
right quadriceps and hamstrings muscle strength at 3+/5 MMT scale.
balance score of 12 seconds TUGT
most postoperative anemia symptoms were resolved
independent level with all of her ADLs
Discussion
The patient’s plan of care was developed based on a combination of her impairments following her right TKA, functional limitations, and goals. She made steady progress towards her stated goals of independence with all of her functional mobility and all of her ADLs, without pain and locking up of her Right knee joint. The patient regained full AROM of her right knee joint and regained muscle strength to engage in her regular activities. She progressed to and demonstrated independence with all of her mobility and planned to resume telecommuting the following week once cleared by her surgeon.
During HH services, the patient was diagnosed with postoperative anemia by her PCP, which is common among surgical patients.7 Following the initial incidence, her vital signs and symptoms were monitored more frequently. Her surgeon and PCP were contacted to report her symptoms, and because the patient was discharged from home health skilled nursing services on 12/29/21, the PT provided education to the patient regarding the possible drug interaction of her iron supplement prescribed by her PCP. Ferrous Sulfate can bind to Doxycycline in the Gastrointestinal tract, which may decrease their absorption and bio-availability. They should be taken 3-4 hours apart to avoid or minimize this interaction. The therapist also provided education to the patient and her husband regarding food rich in Iron to complement her medication.
Several studies have identified the common reasons for visits to the emergency room after TKA. (7-9) A study reported 15.6% of ED visits were for swelling, and 15.8% were uncontrolled pain.8 Another study reported that among patients who had ED visits after THA and TKA, the primary diagnosis in 17.84% was pain.9 To decrease unnecessary visits to the ER, our agency has developed a comprehensive education program for post-op THA and TKA patients. PTs share the information with the patient on the first visit regarding the red flags of infection and possible DVTs; and education regarding pain and edema management. The same information is reviewed on the 2nd and 3rd visits until the patient can verbalize the previously provided information.
This case report highlights the effective management of a TKA patient in the HH setting while incorporating the patient’s unique PMH and postoperative complications. Her exercise program and joint mobilization were modified to accommodate her Ehlers-Danlos condition and her vital signs more closely monitored with the postoperative anemia. Her exercise program was progressed from the initial set more suited for the immediate acute phase to more advanced exercises in the sub-acute phase. She was progressed to independent ambulation without an assistive device on a level surface and with a one-handed device on uneven surfaces.
About the Authors
Babatope Olusina, PT, DPT, Certificate of Advanced Competency in Home Health (APTA Home Health Section). He is a member of the APTA and Home Health section. Dr. Olusina now works for a home health agency in Richmond, VA, but previously owned and ran a Contract Therapy Staffing Company.
Dr. Olaide Oluwole-Sangoseni, PhD, DPT, MSc, GCS, is an associate professor of physical at Maryville University of St. Louis. She is a Board Certified Geriatric Specialist and a home health PT. Dr. Sangoseni is an advanced physical therapy clinical specialist degree in neuro-orthopedics from the University College London, England. She is an APTA credentialed clinical instructor. She can be reached at [email protected].
References
Zhang Y, Jordan JM. Epidemiology of Osteoarthritis: Clin Geriatric Med.2010 Aug: 26(3): 355-369
Jette DU, Hunter SJ, Burkett L, et al. Physical Therapist Management of Total Knee Arthroplasty: Physical Therapy. 2020 Aug; 100(9): 1603-1631
Kremers HM, Larson DR, Crowson CS, et al. Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am. 2015 Sep 2; 97(17): 1386-1397
Inacio MCS, Paxton EW, Graves SE et al. Projected increase in total knee arthroplasty in the United States- an alternative projection model. Osteoarthritis Cartilage. 2017; 25: 1797-1803
Centers for Disease Control and Prevention: National Center for Injury Prevention and Control. STEADI Tools. https://www/cdc.gov/steadi/pdf/TUG Test-print.pdf. Published 2017.
Corrado B, Ciardi G. Hypermobile Elhers-Danlos syndrome and rehabilitation: taking stock of evidence-based medicine:a systematic review of the literature. J Physical Therapy Science. 2018 Jun; 30(6): 843-847.
Perelman I, Winter R, Sikora L, et al. The Efficacy of Postoperative Iron Therapy in Improving Clinical and Patient-Centered Outcomes Following Surgery: A Systematic Review and Meta-Analysis. Transfusion Medicine Reviews, 2018 April, 32:2, 89-101.
Kelly MP, Prentice HA, Wang W, Fasig BH, Sheth DS, Paxton EW. Reasons for ninety-day emergency visits and readmissions after elective total joint arthroplasty: results from a US integrated healthcare system. J Arthroplasty. 2018;33(7):2075-2081. doi:10.1016/j.arth.2018.02.010
Finnegan MA, Shaffer R, Remington A, et al. Emergency Department Visits Following Elective Total Hip and Knee Replacement Surgery: Identifying Gaps in Continuity of Care. Journal of Bone and Joint Surgery: 2017 June 21. 99 (12), 1005-1012.
By: Elizabeth Townsend, RN
People are social beings. With COVID-19 introducing social distancing guidelines and restrictions on visitations, social isolation and loneliness are increasing. A report referenced by JAMA discussed the need for solutions for social isolation and loneliness in older adults. There is significant documentation that social isolation and loneliness are related to a higher rate of major mental and physical illnesses, including:
Cardiovascular and cerebrovascular risks
More depression and anxiety
An increased risk of dementia
According to the National Institute on Aging, people who participate in worthwhile activities with others tend to live longer and have a sense of purpose.
Assessing seniors for isolation and loneliness
COVID-19 has made it difficult for seniors to participate in:
Social gatherings
Communal dining
Exercising in groups
Social programs at senior centers
Volunteering
Home health clinicians assess patients for social isolation and loneliness. Asking patients about their social needs is important to identify who needs assistance, easing isolation and loneliness. The home health agency provides tools or guidelines with questions for the clinicians to ask. Examples of questions to ask:
Do you feel you have no friends or loved ones?
Are you lonely?
How are you staying active?
5 ways to relieve isolation and loneliness
After assessing and finding that your patient is suffering from social isolation, consult with their caregivers and healthcare team —specifically the agency’s social worker—to find ways to relieve their isolation. Daily Caregiving suggests some ways to help:
Encourage a sense of purpose. Suggest activities such as knitting blankets and caps for newborns at a local hospital, making masks for healthcare workers or family members, or writing letters to their grandchildren to encourage them. Allow the patient to have a responsibility, such as taking care of a plant or dog. This would be giving them a meaningful purpose.
Encourage interaction. Encourage interaction with others via phone, computer, or if in person, socially distant, wearing a mask.
Encourage physical activity. Take Into account the patient’s physical ability. They can do gentle exercises such as walking, stair-climbing, yoga, or group exercises via computer. If they cannot get out of bed or are not able to walk, find appropriate activities. Consult with the physical therapy team who can provide resources for exercises for those with limitations.
Assess the food they are eating. Encourage fiber-rich foods like fruit, vegetables, whole grains, and lean proteins. Consult with community services such as food banks, churches, or meal delivery services.
Show them they are loved. Find ways to show that they are loved and needed. Listen to what they have to say. Encourage family members, if they are in the home also, to hug the patient and talk and listen to them.
Social workers can help seniors with social isolation and loneliness
Social workers can ensure that patients have access to available resources. Local churches may have “shut-in” outreach for those unable to leave their homes. They may provide phone calls, run errands, provide food baskets, and communicate by mail with the seniors. Local library programs have online programs and can arrange to have books available for the patient to check out. The social worker can also refer the patient to transportation programs that take seniors to doctor appointments.
Encourage virtual connections for seniors
Advancing States created a resource to help reduce social isolation and loneliness.
If the patient can use a smartphone, show them how to google Earth National Park Tours so they can “visit” the parks and talk about what they saw with others via telephone or with you when you visit.
Put the patient in contact with Well Connected by Covia, who will help them participate in virtual classes, conversations, and activities by phone and computer.
There are helplines for mental and emotional support, which include:
Friendship Line by Institute on Aging- 1(800)971-0016
Happy– a free app that provides emotional support 24/7
National Alliance on Mental Illness Helpline- 1(800)950-6264
Substance Abuse and Mental Health Services Administration National Helpline- 1(800)662-4357
By: Portia Wofford
Home health clinicians play an essential role in caring for patients who are:
At risk of developing sepsis
Recovering from sepsis or septic shock
Home health providers are vital in preventing hospital admissions and readmission among sepsis patients. According to the CDC, sepsis is the body’s extreme response to an infection. It is a potentially life-threatening medical emergency.
Many patients receiving home healthcare services have chronic medical conditions and comorbidities that put them at risk for infection, including COVID-19 and sepsis. According to the Global Sepsis Alliance, COVID-19 can cause sepsis. Research suggests that COVID-19 may lead to sepsis due to several reasons, including:
Direct viral invasion
Presence of a bacterial or viral co-co-infection
Age of the patient
According to Homecare Magazine, approximately 80% of people with COVID-19 will have a mild course and recover without hospitalization. The remaining 20% of patients with COVID-19 may develop sepsis and be admitted. Patients with severe illness will need home health care.
A study published in Medical Care by the National Institutes of Health (NIH) suggests that when strategically implemented, home health care can play an essential role in reducing hospital readmissions for patients recovering from sepsis. According to Home Health Care News, the study points out that sepsis survivors who were less likely to return to the hospital if they:
Received a home health visit within 48 hours of hospital discharge
Had at least one additional visit and
Had physician visit within their first week of discharge
Home health care can contribute to early detection of sepsis
Early detection is critical. For each hour treatment initiation is delayed after diagnosis, the mortality rate increases 8%. Home health nurses can monitor and educate patients and their caregivers on signs and symptoms to report to include. Additionally, home healthcare agencies can provide screening tools that fill the gaps in identifying at-risk patients during transitions from inpatient to outpatient settings.
Home health provides case management for chronic comorbidities
Some comorbidities like Type 2 Diabetes, chronic heart disease, and dementia were associated with sepsis risk in almost all infection types. Those with other chronic illnesses, cancer, and an impaired immune system are also at increased risk. Monitoring can help reduce risks.
Nurses can review and coordinate care to adjust medications, evaluate treatments and interventions, and refer for appropriate treatment.
When it comes to serious complications, our sepsis program effectively:
Prevents infections that can lead to sepsis
Recognizes sepsis symptoms before they become severe
Rapidly responds if sepsis symptoms occur by initiating appropriate treatments and referrals
Follows-up with care to ensure continued recovery
AT Home Care’s sepsis program promotes quality of care and improves outcomes for those at risk for developing or recovering from sepsis.Pandemic Relief via legislation, CMS waivers, and enforcement discretion
CMS permits HHAs to provide all necessary telehealth during the emergency period
Must be physician-ordered and on the plan of care
Does not replace in-person visits (telehealth or telephonic visits are not billable visits)
Allows for HHA to supplement in person visits for patients who might refuse more frequent visits or senior living or other congregate living facilities that might be restricting access to HHA personnel.
The Home Health Face to Face visit may also be provided by telehealth but must be performed utilizing 2-way audio and visual programs.
In an effort to protect patients, some SNF, LTC, hospice, and other facilities are limiting the number of visits that Abode Healthcare staff may make to patients in their care. Some patients are even requesting fewer in-person visits to reduce their exposure to the outside world.
Abode Healthcare understands and joins in these protection measures by offering telehealth visits. In some cases where access has been limited or is desired, Abode staff are utilizing telehealth on a weekly or bi-weekly basis in order to maintain contact with high-risk patients.
In all cases, telehealth visits are meant to be supplementary to in-person patient visits. Telehealth visits should not replace in-person visits altogether.
Telehealth Tools
Our commitment, as always, is to serve our patients as best we can. Our clinical team has been trained in effective ways to utilize telehealth systems to streamline patient care through our own remote access system using the following tools:
Phone: Abode Healthcare staff may conduct remote visits with patients through phone calls.
Video: Abode Healthcare staff may conduct remote visits with patients through Doxy.me. (All F2F between NPs or MDs, DOs must be done through a 2-way type of technology. This is for both HH and Hospice)
me can be utilized via tablets or phone and has been selected by Abode due to the ease of use for both the clinician and the patient/family/caregiver as well as its ability to capture/validate that the tele visit occurred, and its security features.
Though telehealth is never our first choice, it is the right choice during this time. Abode Healthcare continues to partner with providers to preserve the health and wellbeing of all of our patients.
Though telehealth is never our first choice, it is the right choice during this time. Abode Healthcare continues to partner with providers to preserve the health and wellbeing of all of our patients.
CMS clarification on homebound status for COVID-19 patients and those at high risk of contracting:
Non-Physician Home Health Certification Authority
Allows patient to be under the care of an NPP to the extent permitted under state law
CMS utilizing discretionary authority not to enforce rules
Must also check state HHA licensure for any barriers to implement
CARES Act makes this relief permanent, but CMS needs to implement
For more information, contact Jon Wilder.
HomeCare Elite has recognized AT Home Care Williamsburg as a top-performing home health agency for 2018. HomeCare Elite is a compilation of U.S. Medicaid- certified home health agencies annually reviewed by ABILITY and DecisionHealth. The review is conducted using public information evaluating overall performance in quality outcomes, best practices, consistent improvement, and financial health.
Recognition is given to the top 25% ranks home health agencies and further to highlight the top 100 and 500 agencies. HomeCare Elite is unique in a way that it is the only performance recognition of its kind in the home health industry.
Thanks to the AT Home Care Williamsburg team for their continual hard work and dedication to improving the lives of others. Also, thanks to all the families that entrust AT Home Care to provide the care needed for their loved ones. Our team is humbled to be recognized with this prestigious award and hope to continually exceed expectations as the new year arrives.
To find out how AT Home Care services can benefit you or your loved one, please contact us.As a person ages, he or she may begin to lose their ability to live independently due to a variety of physical conditions. These include limited mobility, chronic pain and frailty, as well as typical everyday activities that may become stressors, such as maintaining a household and caring for themselves. Mental health problems may also arise as people grow older. Depression and anxiety are two of the most common mental health conditions.
Health conditions and lifestyle adjustments are inevitable. However, an elderly person does not need to feel alone in dealing with such changes. Whether a loved one needs full-time or part-time in-home care, or just a friendly face to stop in for a visit, in-home care offers a great deal of value that offsets the isolation, depression and anxiety an elderly person sometimes experiences.
Most seniors enjoy the company of family, friends, caretakers and new companions. In-home companionship has a huge impact on the mental health of the elderly. Not only do companionship services provide the senior with much needed interaction, they relieve some of the stress and worry from family caregivers. This allows time spent with family to be more fun and carefree, and less of a stressor.
In-home companionship care includes activities such as:
Playing games, telling stories and help with reading
Crafts, like scrapbooking and collages
Maintaining calendars and organizing social engagements
Planning trips outside of the home
Assisting with personal tasks
Engaging in meaningful conversation
A helpful and friendly companion has a unique influence on a senior’s quality of life. In many cases, after a few visits from a companion, the senior is much more willing to initiate activities and accomplish tasks independently. This sense of self-worth has a significant impact on mental health. For more information on senior companion services, contact AT Home Care today.Assisted living, nursing homes and home health care are issues most elderly persons and their loved ones will be faced with at some point. Whether the person struggles with mental disabilities, physical incapacities or chronic illnesses, most times care outside of what family and friends can provide is necessary. When the time comes to think about options, the process of researching and deciding on an approach can be particularly stressful. Some elderly people may be resistant to change, and would prefer to keep present arrangements because they are comfortable and familiar.
Factors to Consider
Home health care is an excellent way to receive specialized medical care in the comfort and familiarity of the patient’s home. However, before determining if this is the right option for you or your loved one, there are several factors to consider.
Does the person have an accessible, nearby network of loved ones and friends?This is critical because home health care involves the participation and companionship of those close to the patient. When receiving home health care it’s easy for the person to feel alienated, especially if they live alone, and a familiar support system is very important to a successful in home health care plan.
Is the person’s home easily maintained and modified?When an elderly person has medical needs and conditions, it’s important that their living environment is safe. Many times home health care professionals, like nurses and therapists, will recommend some home modifications be made to create a more safe, stable environment for the patient.
Is the person comfortable with having unfamiliar faces in their home?This question might seem obvious, but many times it isn’t until a home health aide, nurse or therapist makes their first visit that the patient feels uncomfortable with the arrangement. Make sure you or your loved one understands who is visiting and why. It’s important to work with the home health agency to ensure there is a good match between the medical professional and the patient.
There are many other key points to consider that are unique to each person. Talk to your family and loved one about the available options of care and try to get feedback in all areas. Together you can decide if this is the right time for in home health care.Independence is an important part of life, but daily human interaction and regular activities are important to a senior’s health and happiness. There is no denying that keeping seniors physically, mentally and socially active can result in overall better health and the ability to live independently longer. Having the right person step in and offer a helping hand is just what most seniors need to achieve their highest level of independence.
A nurse or caregiver can provide an interactive approach to in-home care that stimulates a senior’s natural ability to perform. At a very basic level, in-home caretaking is health care combined with task-oriented activities to encourage a senior’s independence. Overall health and independence is promoted when engaging activities are the focus. There are four main areas of concentration for an interactive approach to in-home care.
Physical Activity
Once physical activity is approved by a doctor, it’s important to remain as active as possible. Sometimes all it takes is a companion to make being physically active more enjoyable. Dancing, stretching, walking, gardening and housekeeping are all suitable forms of physical activity that will improve one’s physical and emotional well-being.
Socialization
Being around others is critical to a high quality of life. As people age, life changes occur that sometimes result in feelings of isolation. By meeting up with friends and loved ones outside of the home, or attending parties and other events, a senior may regain confidence. Additionally, research shows that socializing slows the development of memory problems.
Mental Stimulation
Regularly participating in mind-engaging activities is important for a seniors brain function. Activities such as card games, crossword puzzles, computer activities, arts and crafts and storytelling are all fun and accessible ways to stimulate the brain. These games and activities keep the mind active, and promote healthy mental growth.
Emotional Well-Being
Feeling connected and involved are significant factors that contribute to emotional health. This can include simple things like staying in touch with family and friends, being involved in the community or learning a new hobby. Unlike those included in the socialization category, these are things the senior can do alone, or with friends and loved ones.
An Aging Population And Other Outside Factors Means More People Are Turning To In Home Health Care in Virginia
As the population ages, and hospitals cut back on their stays, more and more people will be looking to home health care as an alternative. Did you know that home care is approximately two-thirds less expensive than hospital or nursing home care? Knowing the options for the continuum of care can help alleviate some of the anxiety that occurs when a loved one leaves the hospital or has increasing medical needs.
The pace and unfamiliar surroundings of a hospital or nursing home can be confusing. Not only is the financial burden of a hospital stay alleviated with home care, studies show that patients with home care often enjoy a faster rate of recovery and the chance of further hospitalization is minimized. The decision to choose a home care giver can seem overwhelming, but the points outlined below should direct you to resources that will make the process much easier. Not only do you want to ensure that the care you will be receiving is of the highest quality, but, also, that the caregiver will respect your lifestyle as well as your home.
Finding Qualified Agencies
Some of the first things to consider when choosing a home health agency are:
Type of care or services that will be needed,
The care giver’s level of training, and
The financial coverage provided by your insurance or Medicare.
You will want an agency licensed by the Center for Medicare/Medicaid. A physician or an Area Office on Aging can help you evaluate your needs and provide you with a list of licensed agencies. In addition, Medicare ranks all the agencies that they certify and conducts performance surveys of each on specific categories of patient care. There are several professional organizations that have established stringent standards to define quality in home care services that go beyond the minimum state and national requirements. Two of the most respected are: The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and Community Health Accreditation Program (CHAPS). Agencies that have attained one of these certifications are the most respected in the home care industry.
Questions To Ask a Home Health Care Agency
Once you have a list of potential agencies, it is time to ask about specific care services, as well as the personal standards demanded of the clinicians.
What type of license does your agency have?
How soon after discharge from the hospital will your plan of care begin?
What is the evaluation process for developing a care plan for the patient and assigning care givers?
Does a nurse or therapist consult the patients’ family and physicians?
How frequently will there be feedback and updates regarding the patient’s progress?
How detailed is that patient’s course of treatment?
How often does the care giver update the family members and doctor?
What procedures does this provider have in place to handle emergencies?
Are its caregivers available 24 hours a day, seven days a week?
Additional Considerations
References should be availableThe area on Aging that covers the Richmond area is Senior Connections
Eligibility for MedicareUS citizens, age 65 years or older, who have contributed to Social security, are eligible for Medicare benefits. Medicare will pay for an unlimited number of visits provided the criteria listed below are met on a continuous basis. Medicaid is for the poorer population and eligibility in Virginia needs to be checked as legislation is currently being altered.
Home Health Care Eligibility under Medicare
Must be homebound. This term means confined primarily to the home as a result of medical reasons.
Intermittent need for temporary nursing care or physical therapy. Examples of this are when a patient suffers from Congestive Heart Failure after a hospitalization; or the need for physical therapy after a joint replacement.
A physician’s order and plan of care need to be coordinated with your doctor and a home health agency.
Private Insurance Usually follows Medicare criteria, although each insurance policy may have different coverage benefits and different co-pay amounts. Call your insurance company and ask for specific benefits and service.
The Types of Services found at Home Care Providers
Nurses (Registered Nurses and Licensed Practical Nurses)
Certified Nursing Assistants
Physical Therapists
Home Health Aides
Speech Language Pathologists (speech therapists)
Occupational Therapists
Medical Social Workers
Companions (sitters) –Personal Care & Private Duty
Taking time to ask a few important questions will go a long way in finding the most compatible home health agency. For a complimentary home health evaluation after discharge from a hospital please call 804 359-3400, and ask for Barbara Wilson, RN Clinical Director for AT Home Care.